I’m new here and certainly feel the need to avoid causing needless strife. The welcome vibes have been great yet I’m aware that our long history as humans and surviving in tribes still pertains and the sense of the “other” always rides just below the surface.
With 42 years of living with diabetes, my resume is deep enough to comment on many topics. Yet I also realize that readers here share in long lived experience and likely have come to different conclusions. But that’s what forums are for: airing it out, exchanging perspectives, and hopefully learning something useful.
Consider potential topic choices:
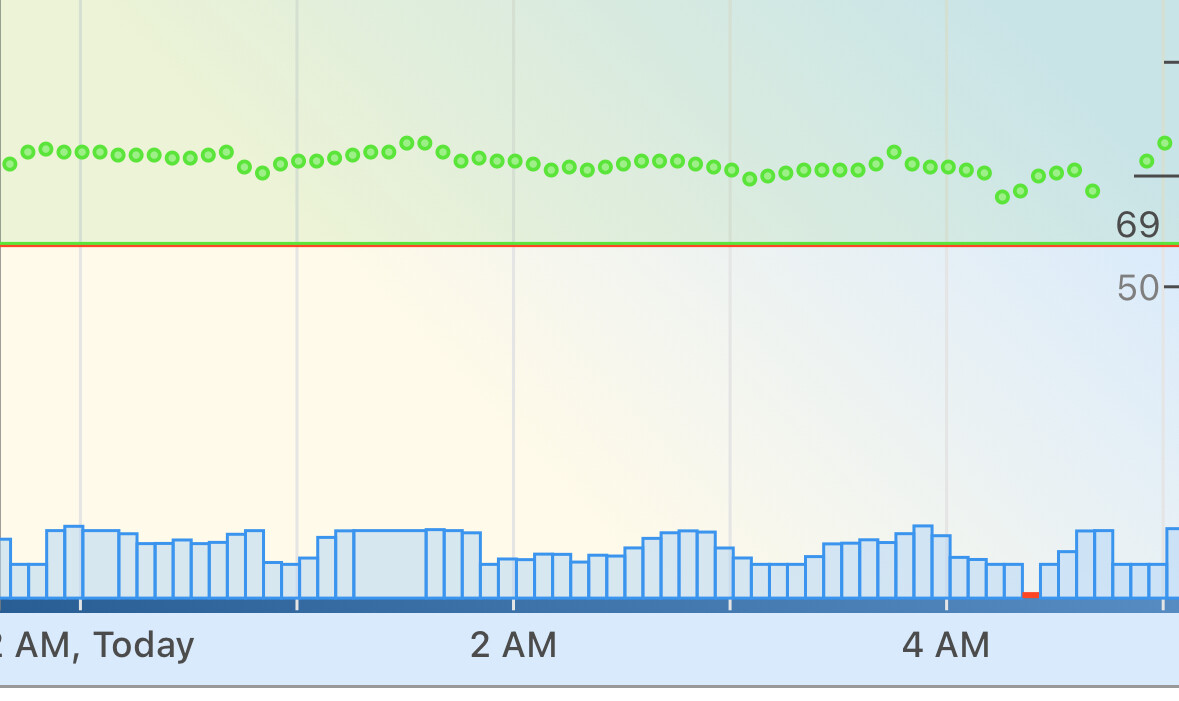
- The numerical assessment of my diabetes data
- How my diabetes technology helps me
- How my way of eating permits “normal” blood glucose levels
- How to socially negotiate with your endo to maintain good access to vital Rx’s
- Why the standard target range of 70-180 mg/dL feels patronizing to me
The numerical assessment of my diabetes data
I’m a diabetes data geek and I make no apologies. I look at the Dexcom Clarity website and the Tidepool site on a daily basis. I surprisingly discovered many years ago, that the mere daily observation of this data mysteriously fueled the long term motivation to make it all work for me.
Yet I know that this topic can easily be dismissed by readers as being a trite exercise in ego-stroking. “Look at my 24-hour no-hitter with tight time-in-range limits!” My motivation truly is one of sharing with others diabetes success as way to inspire them to the same experience. Getting the tone right is critical and for me it’s still a work in progress!
How my diabetes technology helps me
I’ve used a pump for 39 years, a CGM for 16 years , and an Automated Insulin Dosing system for 9 years. And I believe that I’ve found every way to break these gadgets but I haven’t killed myself yet! My experience is deep and I have much to share but fear coming off as pedantic, a self-appointed teacher propped up behind a podium. I’m also aware of many readers here who share my deep experience but don’t necessarily share the lessons I’ve learned.
I can reveal statistics and graphs that support my expertise but there’s always the danger of that being perceived as an ego-exercise.
How my way of eating permits ‘normal’ blood glucose levels
This topic represents a true minefield for a diabetes writer. It’s a simple truth that no-one likes being told what s/he should or should not eat, me included! Sometimes, even the simple suggestion of altering one’s way of eating creates an instant tempest.
The hard truth of diabetes, however, is that it is a breakdown of our fundamental ability to metabolize nutrition. We’re forced to inject insulin peripherally (much less than ideal) and balance out the timing and amount of nutrition we consume. It’s also a stubborn fact that carbohydrates comprise the largest driver of insulin needed. We must address this reality or go home!
This explanation seems simple enough to me but I’m embarrassed to admit that it took me 28 years for the practical reality of that to sink in. I finally took action in 2012 and started to limit carbs in my diet. I lurked for two years at TuD watching the “carb wars” evolve before I acted. I don’t believe I would be writing this today if I hadn’t acted then!
We diabetics are touchy about how we eat! In fact, all people are touchy about how we eat!
How to socially negotiate with your endo to maintain good access to vital Rx’s
This point, at first, seems non-controversial. The disparity between our deep lived experience and the endo’s common inability to understand and respect our depth of knowledge creates this diplomatic challenge. However, not all endos are like that and I can see the immediate defense coming now.
For me, I’ve had to pick and choose my words carefully, four times/year for 42 years! It’s not really their fault; no one who doesn’t live with insulin dependent diabetes all day, every day can truly get it.
Why the standard target range of 70-180 mg/dL feels patronizing to me
I wrote a post at TuD several years ago with this topic. While it was provocative, it did not endear me to everyone. I lost a few valuable relationships over that piece.
I value normal blood glucose levels. In any scenario, I think that setting valuable targets, aspirational ones, is how to play this game well. I know why the clinicians set the more moderate glucose targets. People with diabetes have a hard time aiming for better. Normal blood sugars seem hopelessly out of their reach. And the mind game is important!
What these clinicians need to acknowledge is that a significant minority of people can and do shoot for normal blood glucose. Check out the FB community TypeOneGrit. You’ll never hit a valuable target if you don’t aim at it first!
Anyhow, I’ve given a good deal of thought about what to explore in diabetes topics. The challenge feels daunting to me as I’d like to earn/keep your respect. Let me know your thoughts.