Right. Perhaps this is my only hope.
But if there are people who manage on MDI, then surely i can? i’m loath to admit defeat, particularly when i see others seem to manage just fine.
One halfway house: can I use a pump overnight, and revert to MDIs during the day?
Or is it one or the other?
No - but perhaps i should. Currently using jelly babies (or equivalent) or pure orange juice (in any attempt to reduce the amount of junk i’m poisoning myself with while treating hypos). Previously i’ve found little difference in time to react to most types of carb (brown rice/white rice/apple/juice/jelly babies) - they all pretty much take the same time to cause a movement, and that movement is all the more sudden and extreme the longer and lower i have been, which makes dosing the sugar fix extremely difficult.
While a lot don’t like them I find that glucose tablets are best for treating hypos for several reasons. One, they are very fast, especially if you drink water after swallowing, Two, they are exactly 4 grams of glucose, so easy to measure. Three, they are not yummy - some might find this a disadvantage, but it helps me to not overdo.
There is the 15/15 rule for treating hypos. Eat 15 grams (4 tablets) wait 15 minutes and check BG. If still low repeat. Now we are all different, and with a CGM I have learned that I might be best served by 4 grams (1 tablet) or 8 grams.
It pays to carefully meter consumption and the effect it is having on BG. In the past, I would treat hypos by overdoing, setting me up to a roller coaster of BG.
On another topic you brought up - steatorrhea (fatty stools) - We with diabetes regardless of type are at risk of exocrine pancreatic insufficiency (EPI).
We tend to forget that the pancreas is a multipurpose organ concerning ourselves with the endocrine functions which are only <2% of pancreatic mass. The bulk of the organ is exocrine, creating and distributing digestive enzymes to complete the digestion of all 3 macronutrients.
Newer testing methods determine around 12.7% of diabetics have EPI. This is slightly higher in those with T1 than T2. The prevalence of EPI tends to increase over time since diagnosis with diabetes.
I don’t think that even if your exocrine pancreatic function has declined a bit, that this is causing your yo-yo BGs. What is important is besides not digesting fats well, the fat soluble vitamins may be malabsorbed.
There are guys who can bench press 800 lbs, but that’s no reason to suppose that I could achieve it. Our bodies’ capabilities and requirements are individual. YDMV means exactly this: what works for someone may not work for someone else.
It’s possible to mix pumping and MDI. Some people use a long-acting insulin for their minimum basal, and have a pump add extra during times of day where it is needed. Some folks use injections for bolus and pump their basal. For myself, once I started pumping for variable basal, I always had pump insulin available for bolusing and corrections, so I stopped carrying syringes and vials. (But I have an emergency syringe in the car in case I ever want to pull insulin out of a failed pump to give a manual injection.)
In your case, since it seems that your overnight basal requirement is higher than your daytime basal, it would be possible to take a tresiba dose to cover the daytime basal amount, and set the pump basal to add the extra amount as needed overnight. If you do that, you might even find it more convenient to just let the pump handle the daytime dosing too.
Yes, of course, I remember you! I recall we had a zoom call to troubleshoot your Libre issues for xDrip+. Thank you for your kind words.
YDMV is quite true. Hence, one must go slow and test each change recommended by someone else, as the change may not result in the recommended expectation. And worse, as I know you are experiencing now, YDMV even changes for oneself sometimes daily!
It is difficult to troubleshoot why you are suddenly (for the last few weeks?) rollercoasting like you are. I agree with you in that it is hard to break the rollercoaster cycle once it begins. I found the only way to get back on track was to minimize what I ate (carbs, fats or otherwise) by sticking to known foods that had low glycemic effect, while continuing with daily exercise. I know you want to maintain your weight so maybe this won’t work for you. There was another thread on this forum started by @CarlosLuis about the need to add calories and it was suggested that he add Boost or Ensure or other drinks to his diet. That may be something you could try to add weight.
I found MDI very difficult to achieve a normal BG range, which was my goal. I think MDI requires more work simply because one needs to perform the physical injections, whereas the pump will automatically perform the micro injections according to its integrated CGM and loop algorithm at each CGM reading. If you want to try MDI with an open loop system, you could install AndroidAPS on your Android phone. I used this app even before I was on the pump just to get familiar to loop systems. Using it in open loop mode is quite a bit of work since it requires the user to give MDI injections manually but it will give you an idea of what a closed loop system can do. AndroidAPS happens to support OmniPod, among other pumps, and supports xDrip+, on Android.
This is extremely interesting advice - i have procured some Dextro tablets and will see how i get on.
However, i don’t know about you (or other members) but do you find you have different degrees of hypo? if i’m down in the low 2s, generally speaking 4 tablets isn’t going to cut it, particularly at night. typically, i’ll have some snack, and it might (eventually) get me back up into the 3s/4s… but then i quickly sink back down again to the 2s, and i get woken up again. This can sometimes happen 3/4 times, by which time, frustration sets in, and i end up overdoing it, and then zoom up to 20. (incidentally, this would appear to suggest my 18u of basal is too high, and it probably is for that night… but other nights i have the opposite problem and keep being woken up too high…!)
So… does this 15/15 rule apply however low one gets? Or is this for a 3.0 hypo and needs tweaking for hypos that go down into the 2.0s (or 1.0s!) ?
Again, very interesting. I am currently taking some ox bile to see if insufficient bile secretion is the cause of my fat malabsorbtion, but i’m not seeing any difference a couple of weeks in, so I am wondering whether this could well be EPI rather than BAM (Bile Acid Malabsorption). In which case, perhaps a lipase supplement could be in order? Generally not a great fan of lifelong supplement requirement, on top of everything else. I wonder if there are more natural remedies?
Interesting that you think this isn’t the cause of the yoyo’ing… rather just another annoying problem that needs addressing.
Either way, many thanks indeed for your thoughts and insights here, which have been extremely valuable.
But i’ll always have the pump attached? i guess it isn’t practical to be attaching it each evening and in reality you just leave it on.
For the last year or so, along with my daily 18u Tresiba in the evening, i took to taking a dose of Humulin I also, to try to arrest my 2-4am highs, varying it depending on activity levels and meals (generally 1-4u). This worked for a while, but during this perioc of yoyo’ing (which might finally have started to subside) it seems to have stopped.
Thanks for coming back, @Trying. For me, this is the most frustrating part of dealing with this disease. One (or at least I) can never work out the rules of the game as they’re continually changing…which means (at least for me) any attempts to manage it are really only guesswork. Which is really quite depressing.
Indeed. I think you’re right, when yoyo’ing uncontrollaby, just stop eating. I can’t really do that given my exercise and build.
Right - but they’ll have plenty of carb in them i guess? so when aboard rollercoaster, i suspect these won’t help me get off
This is an interesting idea - i’ll have a look at this. But wouldn’t it ask me to inject very small increments (very frequently), that aren’t possible with my (or anyone’s) pen? i thought that was largely how the system works, by microdosing semi-continuously, at a user-variable or automatically-adjusting rate?
It depends on the pump technology. With an Omnipod it’s always attached. With a tubed pump such as the t:slim it’s easy to disconnect and reconnect as needed: The infusion set stays in, but the tube is easily disconnected, so the pump and tube can be put away and only the small infusion set remains on your body continuously.
This is common because the glucose is fully absorbed in a short time, whereas subcutaneous insulin acts for several hours. One trick is to treat a low with a fast carb to get to a good level, and after a few minutes add a slower food to provide continuing digestion to cover the continuing insulin action. Peanut butter is a common example of a slower food.
It’s simply a dynamic activity, like managing the speed of an autombile with the accelerator pedal, or managing the heading of a sailboat with the tiller, or putting a stringed instrument into tune. Dynamic circumstances are continuously changing the inputs needed to keep steady. With an auto it’s hills and wind and snow or rain or soft ground. With a sailboat it’s wind speed and direction and the action of the waves. With the instrument it’s temperature and humidity. In all these cases, you can’t just set something correctly and expect it to continue to be right, the system is dynamic. For blood glucose management, sometimes the term “sugar surfing” is applied to the numerous small adjustments with insulin and carbs to keep guiding the BG into range.
I don’t think I could function mentally/physically at 2mmol/L certainly not at 1.0.
I don’t know if anyone has suggested glucagon to cause a release of glucose from the liver. Two, that I am aware of are BAQSIMI (inhaled) and Gvoke (injected). This might be something to take up with your endo. A lot of people with type 1 have Alpha cell disfunction. The Alpha cells and Beta cells have insulin and glucagon receptors respectively. With the Beta cells dead this relationship no longer exist. Oh the Alpha cell insulin receptors does not respond to exogenous (injected) insulin.
The 15/15 rule is not set in stone. It is best to see how you respond. I am type 2 on a pump and have some Alpha response, My hypos are almost always exercise induced. An example from tonight, I was stationary cycling watching TV. This nearly always causes a drop 30 to 40 minutes in. When it drops to 3.5 I will eat 2 (8grams) of glucose tablets, drinking water after chewing and swallowing. After I finish pedaling my BG will often rise, sometimes needing a bit of a correction bolus.
On the odd times that I go low on long bike rides, depending on how long to the end, I may do the full 16g of glucose and if there is another 45 minutes of riding to the finish, I will eat something more long lasting - peanut butter crackers (21g) and/or a nut bar (9g).
You have to experiment a bit to learn what works for you.
I don’t think there are any way to supplement exocrine digestive enzymes with food choices. These enzymes are natural even if they are in pill form.
Best to run a little experiment to see how your own body reacts. Some time when your BG is safe and relatively stable and you don’t have meal insulin working on you, take 1 glucose tablet and see how much it raises your BG within a half hour or so. So 2 tabs would double that rise, 3 would triple it. After running that experiment you’ll know how many glucose tabs your body needs, depending on how low you are.
Thank you. This is of course sensible and reasonable, and i shall try precisely this. My biggest challenge remains the instability and nonlinearity of this relationship. One day, while everything is ticking along okay, one tablet may cause me to rise by 2mmol. But when down in the low 2s, it likely (at least in my experience) results in a very different rise - likely 0.5-1mmol. The nonlinearity and it’s volatility is what makes, for me at least, treating hypos (and not shooting higher later) so very difficult.
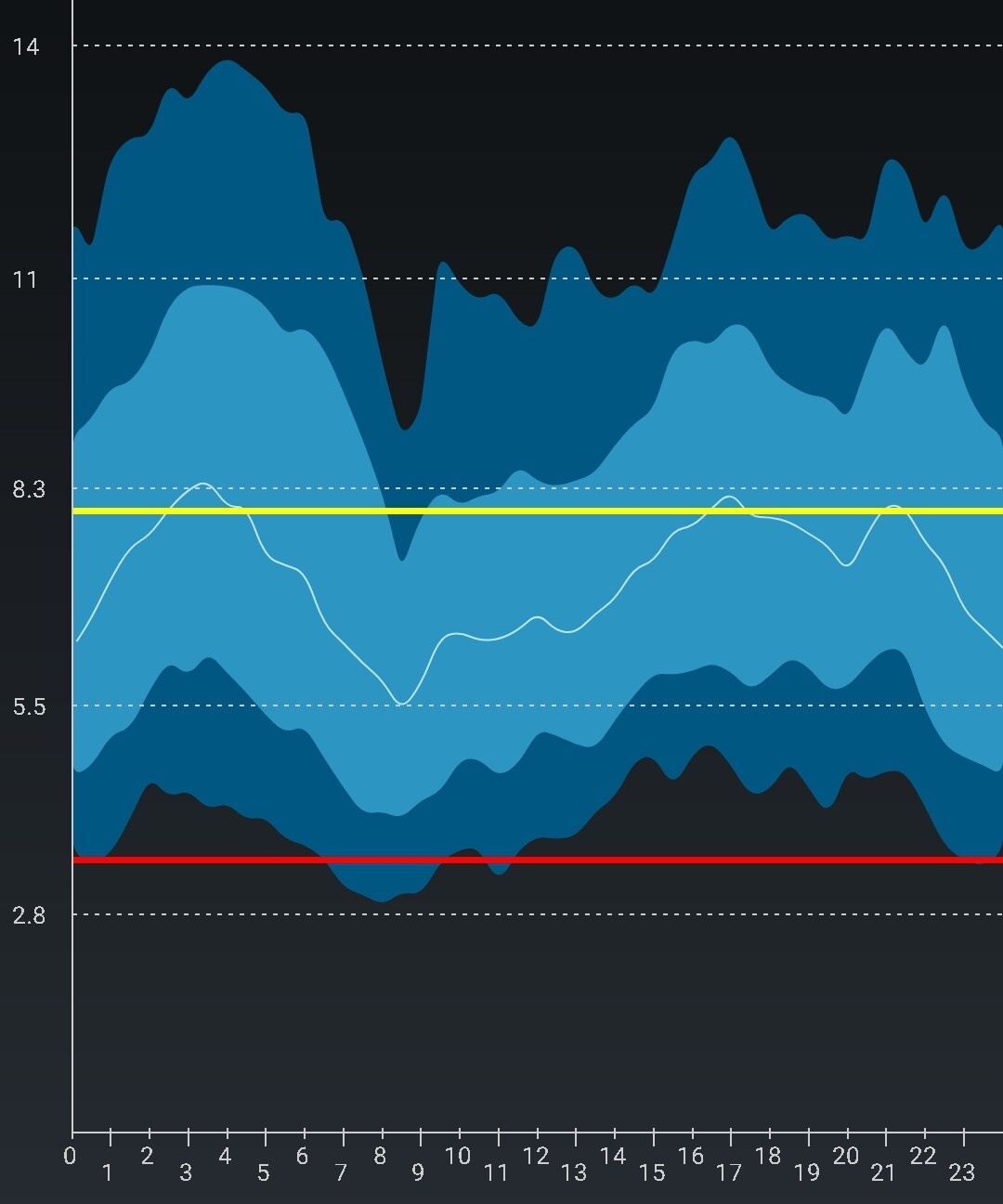
I wonder whether everyone else follows a fairly comparable 24hr pattern of BGs ? Below is my 90d average. You can see as i go to sleep, i rise (sometimes, and recently, violently), and then fall back down as either bolus or Humulin I (from previous evening) or Tresiba kicks in. I then rise after breakfast (pre-bolussing when getting on the Tube or running around at the office just feels too risky for me…too much can go wrong) and then rise into the afternoon/early evening.
I only really come down after exercise during the 7-9pm window and aggressive dinner bolussing… i then start rising again after going to sleep, and the pattenr repeats.
You’ll see the range is wide, as there is much volatility around this general range.
I can discuss that. The thing that makes me go low is that I have taken more insulin than my body actually needed. And I know that the subcutaneous insulin that sent me low is working to carry glucose out of my bloodstream for several hours. So when hypo, I take glucose to raise my BG level, but there continues to be excess insulin, and it needs to be handled. With MDI, extra carbs would be needed to counteract the remaining excess insulin. For me, it’s easier because I’m looping, so the software already would have instructed the pump to stop delivering basal insulin when my BG started trending towards a low, so that helps automatically counteract the excess. I guess how much extra carb is needed for the remaining insulin action, and if I take too much the loop software will see the rising BG and gradually add insulin to counteract it.
Perhaps, but it would be coincidental, wouldn’t it. Because the pattern in the BG graph is not showing your body’s insulin requirement, it is showing the consequence of many counteracting factors: times of insulin dosing, insulin types and quantities given, times and quantities and glycemic properties of food eaten, the activity and stress levels, and all the other individual factors that affect your body’s BG. The graph shows how all those factors have balanced out against each other with the way you live.
I can say that after adjustment, a closed loop insulin dosing system will tend to flatten that graph, because every 5 minutes it is making a decision to give or withhold insulin in an effort to push the BG in a good direction. Even without closed loop, with a pump one would tune the schedule of basal insulin to give more during your peak BG hours at night and afternoon/evening.