Making dosing decisions with a toddler is especially difficult, often resulting in dramatic highs and lows. I cannot seem to get the A1C of my son lower than the high 7’s. I am curious as to what others can accomplish and the strategies behind it.
Our lab-measured is usually between 6.6 and 6.8. His Dexcom average is lower though – usually says between 6.0 and 6.4.
However we are using openAPS which automatically adjusts basal. While it isn’t perfect, I would say the system keeps him mostly below 220s in the days and (unless his settings are wrong), will pretty much always keep him under 200 for most nights.
He was also diagnosed at an A1C of 7.2, and my understanding is that there is a little bit of metabolic memory involved – in other words, if you’re diagnosed at a fairly low A1C it is often a little easier to keep to that range.
For us, what’s really challenging is that he’ll usually have 2 weeks to a month of good BGs, and then have a few days of really, really awful BGs (sometimes even getting up into the 400s) – and those spikes really are enough to ensure you can’t get down really low. Those spikes aren’t always the same thing either – maybe it’s a sick day or a hormone thing. Maybe his site is bad. Maybe I’m out of town and someone else is managing him. Maybe he went to sleep with his pump suspended.
I think it’s possible to reduce the day-to-day variability quite a bit but I think those random spikes are just hard. My long-term goal is to reduce how much time it takes for us to identify the cause (or probably cause) on some of those spikes and then cut down how long they torment us.
I think our strategies are basically: Using the artificial pancreas, and bolusing anytime I see a rise rate over a certain threshold – no matter what BG number he’s currently at. If he’s really high, I will bolus way way more than I think is needed, just to bring him down, while mentally calculating how many carbs he needs to eat in about an hour or two to compensate for the overbolus. So if his usually ISF is 1:240, when he’s at 270 I may give him 2 units of insulin if he’s rising super fast, knowing full-well that is probably at least a unit more than he needs. And then I just make sure I have enough food to feed him over the next 2-3 hours to soak up all the extra. I mean, there’s more to it than that, but that’s the general principle.
I also think that if I were NOT using an artificial pancreas my strategy would be to make use of extended boluses for meals and temp basals like they’re going out of style.
1 Like
Our last checkup we turned the corner from the 7’s coming in with a 6.9. According to our current data, we now have Liam at 6.6. We struggle with the unexplained days like Tia has referred too…doing things exactly the same as they have been done hundreds of times before yielding some crazy high, or some low because BG’s never rise, or whatever. But we are feeling really good about our direction, what we’re doing, and as I indicated yesterday in a post, we’ve successfully gone 1 week and 1 day now without 1 severe low. We also have a very low, “low” percentage. Our 7-day A1C is 6.4, our 30 day is 6.5 and our 90-day is 6.6 currently.
What we do:
Beginning in the morning (whenever he wakes up…which, during the summer, can be as late as noon)
Bolus him for w/e he is going to eat, but set it up as an extended bolus, over 1 hour. 0% up front, and the remaining amount over 1 hour. We then feed him 30 minutes later (when there is 30 minutes remaining on the extended bolus). We also do a “super bolus” (Thanks @TiaG). This is where I bolus him for more food than we are going to give him up front and the extra portion is to be given when he’s in decline, nearing 100. For instance, for Liam, he usually eats 1/2 whole grain waffle, and 1 cup of milk. Our total bolus amount will be 20. 8 for the 1/2 waffle, 6 for 1/2 cup of milk RIGHT NOW, and 6 for the 1/2 cup milk that he will drink when he’s coming back down and near 100. He only eats 14 carbs up front in this example, and the remaining 6 grams comes later.
We also turn on his temp basal at the same time. We have a few configured but the two we use most often are .50% more, and .95% more. Which of these two we use depends on how he’s been rising or falling throughout the day. Some days I start out with 95% more basal, then if I see his sugars aren’t rising as much as usual, or at all, then I switch to 50% more for the remaining meals for that day. I always set the temp basal to run for 2 hours unless he’s eating something like pizza or pasta…when he’s eating something high in starch, I set this temp basal for 4 or 5 hours.)
So Liam eats his breakfast at the 30 min mark on the extended bolus. We then wait to see what his sugars start doing. As soon as I see one of two conditions having been met, I “micro-bolus” him (thanks @TiaG). This is typically a term, I’m learned, that’s associated with children with the open APS, but I’ve adopted that term anyway because it’s what I’m doing. If Liam is double arrows up at 140 or higher, I give him .25 bolus. I then wait. If he continues double up over 180, I’ll give him .15 more. I don’t give anymore to avoid a crash. Those two micro-boluses slow him down usually before, or just over 200. He then declines.
When he comes back down to near 100, we give him the other 1/2 cup of milk that he was previously bolused for.
We pretty much repeat these processes for lunch/dinner, and just keep a watchful eye on his sugars throughout the day and when/if he goes down toward 80, we’ll give him cheese crackers (2.5 or 5 carbs worth) or a bit more milk (1/4 or 1/2 cup depending on the drop) to raise him up enough to last through until the next meal.
Besides these things, the only thing we’ve changed are updating his “low” alerts at night, moving them to 100 so that we can pre-empt the lows, instead of hearing the alarms when he’s already low.
1 Like
I’ve also only started setting his Low alerts to 100 during the nights in the past 1 week, or a little more…I believe this is going to SIGNIFICANTLY cut down on both the low, and the severe low percentages for us. Also, I just looked at the updated data this morning and our 90-day average has now moved down from 6.6, to 6.4%! We are super stoked that this method we’re using seems to be working for us right now.
Here’s some screenshots of our data for Liam using our method.
Liam’s 7 day AGP (138 ~ 6.4% A1C)

Low and Severe Low Percentages for the past week

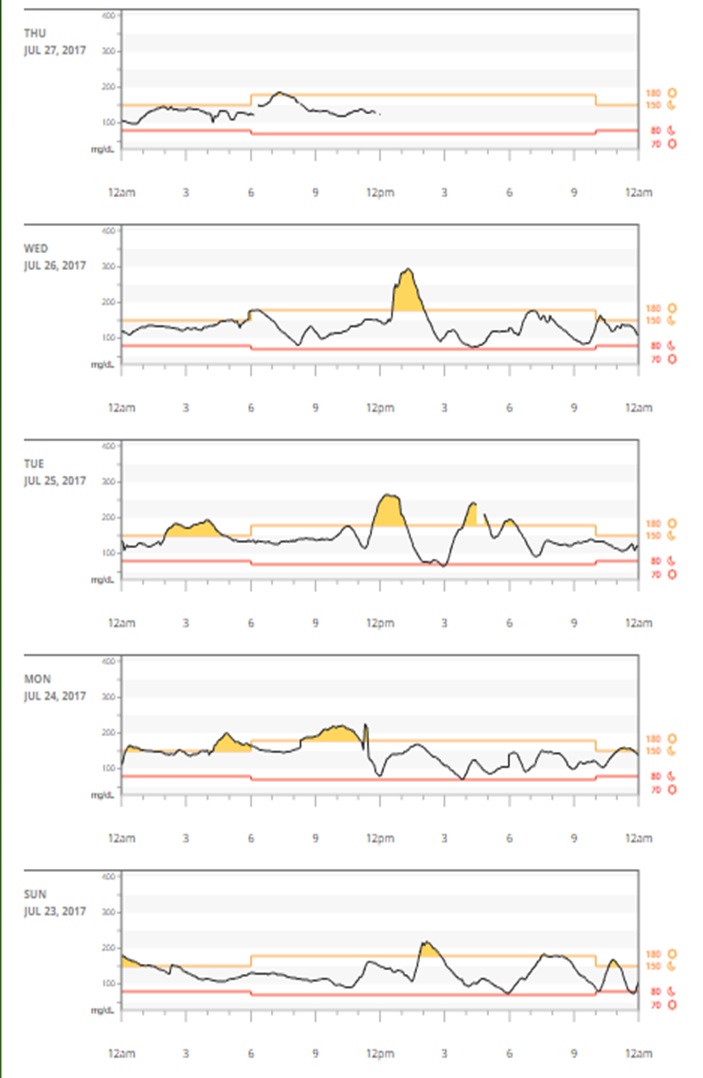
Daily data for the past 7 days
Updated 90-Day Averages / ADP (137 ~ 6.4% A1C) (Notice the high Serious Lows and Lows…we feel certain setting our alarms will bring this 90-Day average down by a lot over the next month or two.)

1 Like
Great results!! So happy for you guys. Seems like you’ve really gotten into a groove that works well for Liam. And it’s just so much less stressful day to day when you’re not dealing with as much of a roller coaster, right?
2 Likes
Yes, and I owe a lot of our success to you, @TiaG. Without your helpful insights and suggestions, we would be far from where we are today. I am forever in your debt! I just hope I can help others as you have helped us.
2 Likes
@Bradford, have you read the book Sugar Surfing? I think it has some great tips for how to manage BGs. Not all of them work great for a toddler but at least a few I really like, like microbolusing and micro-carbing.
To prevent lows, I think you need to have some preset thresholds where you treat lows based on Dexcom that are above the true low, with enough margin to allow your son to bottom out before hitting the low. For us, these thresholds are less than 80 horizontal arrow, less than 95 diagonal downward arrow, less than 125 straight arrow down and less than 155 double arrows down. This is not perfect but just agreeing on these pre-set thresholds helps I think. Sometimes it’s too aggressive to treat a 124 straight arrow down, and sometimes it’s not fast enough to treat a 95 diagonal down. But most of the time it keeps him from hitting the lows…which means it’s easier not to overtreat or cause a rebound high.
Also, who is the primary person who is managing your son’s BG day-to-day?
For us, another thing that’s important is continuity of care. For instance, my husband and I have very different styles – which both mostly work out. He’s much more hands off and reliant on the openAPS algorithm, I’m much more likely to preempt the algorithm.
But the worst results happen when I make a change or execute part of a “BG maneuver” so to speak, and then fall asleep or go to book club or whatever and my husband has to take over from me partway. Or like last weekend, when we were at a swim party with both kids and so each of us are chasing after the kids and making BG decisions on the fly for the two seconds Samson is within grasping distance… there was definitely no coordination of care there.
So having some agreed-upon protocol for hand-off is important. We are still working on that  . (For instance, last night I lowered Samson’s overnight basal to prevent some 3am-4am lows, and then Mitch was on the overnight. But he fell asleep on the couch without all the alarms nearby and Samson was over 200 for several hours of the night. Oops.) But many of our lows and highs I think can be attributed to these “unforced” errors, if you will. So having a seamless care transition process I think would be ideal.
. (For instance, last night I lowered Samson’s overnight basal to prevent some 3am-4am lows, and then Mitch was on the overnight. But he fell asleep on the couch without all the alarms nearby and Samson was over 200 for several hours of the night. Oops.) But many of our lows and highs I think can be attributed to these “unforced” errors, if you will. So having a seamless care transition process I think would be ideal.
2 Likes
Wow! Great information. My wife is the primary caregiver and we, too, tend to have differing styles of treatments. I have read “Sugar Surfing”, but can be a bit tricky with a toddler. With me being at work all day with my wife at home, I sometimes find that a suggestion for trying a different strategy can seem like a personal attack, rather than a simple conversation. Me seeming like a “backseat” caregiver during the day doesn’t help–despite good intentions. I really appreciate the detailed descriptions of your strategies. It is very easy to feel like a failure when your meticulously calculated plan totally falls apart. We seem to go through waves of “everything working well” to “back to the drawing board”.
2 Likes
@Bradford, this is our life’s story and I expect this to be the case until Liam is out of his toddler stage. What’s working amazingly right now can (and most likely will) not work a few weeks from now. It’s why we just celebrate the really good weeks and keep our chins up on the bad weeks.
1 Like
Well - Here is where all the smart parents of toddlers disappeared to from that other site… ![]()
Our 22 month old’s last A1C about 3 months ago 7.1. We are still on MDI with Humalog/Levemir and there is very little insulin control with his small doses. His BG meter average runs about 150 right now, which I have to say isn’t too bad all things considered.
At this point I am at a loss for strategies as the BG is completely random ![]() . As an adult with T1, my strategies do not work for my little guy. For example two nights ago he was 50 in the middle of the night and we were giving glucose and last night he was 270 and we were giving insulin. You can’t win for trying. I keep telling myself that as he gets older it will be easier.
. As an adult with T1, my strategies do not work for my little guy. For example two nights ago he was 50 in the middle of the night and we were giving glucose and last night he was 270 and we were giving insulin. You can’t win for trying. I keep telling myself that as he gets older it will be easier.
My wife is the primary caregiver (as she is at home while I work) and feels this way a lot. I am working on convincing her that a pump/CGM is a good thing but she is hesitant because there is not a lot of real estate on his body yet. I figure around his second birthday we will probably make the switch.
She has a pretty good strategy where she gives insulin at meals and then adjusts carbs at meals and snacks based on BG testing. For example if he is running a bit high it is a no-carb snack but if he is ok then a few carbs. We probably test every 2hrs during the day. This is similar to how @TiaG and @ClaudnDaye do with stretching meals out.
@ClaudnDaye - numbers looking pretty awesome!
3 Likes
From one parent of a T1 (ours was diagnosed at just over 2 years old) to another…do yourself the biggest favor ever and get your child on a CGM first and foremost. The CGM provides updates of your child’s BG levels every 5 minutes. I’ve posted this before, but previous to the CGM I wouldn’t sleep and when I did, it was only an hour a night or so. Even when he was sleeping peacefully and his BG’s were great, in my mind, all i saw was my son lying there, still…which, to me, meant he could be dead. So I was sticking him so often it was crazy. The CGM allows more sleep each night. Now I can just roll over, look at the reciever and if the numbers are good, go right back to sleep, instead of needing to stick him to find out. It’s the first, and best piece of equipment I would recommend every diabetic use.
We had Liam (our son) on the CGM first, shortly after diagnosis, and about 6 months later, he was put on the pump – we use the Omnipod. There is plenty of real estate! If that’s your only concern, I would just do it. My son hated the MDI and with the pump, it allows us to administer all his insulin remotely and we only have to do a changout once every 3 days, instead of 3 to 8 shots per day (depending on his BGs.)
We are here to give you guys any answers you need or any help! The people in this community were here for me when Liam was first diagnosed and they really showed me the ropes (which I’m still learning), but It’s amazing how quickly we learn when our children’s lives depend on it.
PM me anytime! Have you seen the video I made of our 1 year anniversary change-out of Liam’s CGM and pump? If not, check it out here…this will give you an idea of how much real estate these things take on a little guy.
Note: After 1 year, he still didn’t like the change-outs, but he also hated the many shots he got each day, so we just deal with the crying. He still cries, and we try to do as many of them as we can in his sleep (60% of the time we’re successful in doing full change-outs while he sleeps), the other times, he wakes up and cries, but we comfort him until he’s OK again.
1 Year Anniversary change-outs
BTW - you guys are doing great! That’s a super A1C!!
1 Like
Even if you don’t go with a pump, I definitely recommend the CGM. Averaging 150 for a 22 month old is really great–especially without a pump and CGM! We had the same reservations about “real estate” on such a tiny little body. My wife was extremely resistant to the idea of attaching a piece of technology to his body at all times, but she wouldn’t have it any other way now. My boy was 2 years old when diagnosed, so not impossible. Glad to see you here @Aaron. Just curious, how did you ended up finding FUDiabetes?
1 Like
Yes, we weren’t hesitant because of all the wonderful advise from you guys. We knew we wanted to manage his BG’s as good as we could, and MDI’s just didn’t provide the tiny doses that toddlers need. And the CGM’s really did save us both a lot of sanity. You’ll find, as @Bradford indicated, that you and your wife will NOT regret it…there is plenty of real estate (we use both arms alternated for CGM and side/upper thigh and upper bottocks for the PODS - rotating directions of the pods), and these devices really makes diabetes management so much easier for not only you, but your child.
1 Like
Hi @Bradford - Someone on Tu posted a link to this forum recently in a thread complaining about SPAM. The post on Tu quickly disappeared but not before I saw the link.
@ClaudnDaye use an Omnipod and Dexcom CGM so I know how great they are (and I have a spare CGM receiver too… so we can start any day). Thanks for the video - I think that will help. Our son does not cry or get upset for shots. When I say “can I have a finger?” he sticks one up for the BG tests. We are lucky that way.
Our son also has no problems at all with finger sticks. He never has minded that part of it - he decides which finger we use. But any other “change out”, he does mind. Our kids certainly are strong through all this!
1 Like
Blockquote
In the video your son sure is a trooper with the CGM and Pod changes.
I get my other kids to do the CGM needle insertion for me some times for fun (but not my T1 toddler) ![]()
1 Like
Aaron, welcome! Glad to see you here!
My son is older (now 12, diagnosed when he was a young 11), so I do not represent quite the same class of parents – but I would also 100% endorse a CGM. It has changed our lives, and greatly improved our BG control.
We recently lost our Dexcom for 3 weeks and the difference was notable. I get many more hours of sleep when he Dexcom is on and working well ![]()
Kudos to your wife and you for doing so well with your toddler. You parents with toddlers have the hardest job of us all, both physically and psychologically.
2 Likes