Oh, we are talking about PDMs!! I don’t use PDMs so i can’t speak to those.
2 Likes
@Marie I forgot you were also on Omnipod Dash.
2 Likes
My son Kaelan has been on Omnipod + Loop (“Omniloop”) for 3-4 years.
I don’t think he would consider switching back. That said, it is very far from perfect. It gives him a lot of work.
The highlights: he is in college now, which caused him to lose close to 1% in A1c, from about 5.8-6.0% while at home to 6.8-7.0% in college. But his last A1c was 6.3%, so it has improved.
The big boon for him: these days, very few lows at night (for him), no more than 3-4 times per month. That was the big prize for us with Omniloop, better night safety. That part has paid off but required a lot of adaptation from him.
10 Likes
Congrats on Kaelan’s success with the DIY Omniloop. Lows at night were the bane of my existence before I changed my way of eating and before I started on the CGM. Congrats to Kaelan for his improved 6.3% A1c! Diabetes is a tough foe, especially for the young, adolescent, and young adult.
I think that anyone who is capable of treating their diabetes with DIY AID tech is smart to take advantage of it. Good for him!
5 Likes
I don’t think a poll on FUD, or TuD for that matter, will tell us very much. There are statistics for the number of diabetics who use a CGM and that is a prerequisite for an AIDS. This is from the period 2017-2019:
- “Among 11,469 type 1 diabetes patients, 48% were CGM users.” Then, from the table below that quote, 63% of the CGM users (and 20% of the non-users) also used an insulin pump. So at that time only 30% of US T1s could be using an AIDS.
Going to T2s this paper provides numbers, this time from 2021:
- “Among 30,585 adults with type 2 diabetes, 13% had used a CGM.”
They didn’t have the data for insulin pump use:
- “Finally, we were unable to reliably determine which CGM users were also using an insulin pump with EHR data.”
My feeling is that both numbers will be an overestimate because of sample bias away from people who are uninsured or unable to afford to use insurance. The T1 figure is significantly out of date. The following UK data is helpful when working out how things are changing over time:
- “The proportion of pregnant women, with type 1 diabetes, using real-time CGM technology increased from 47% in 2021 to 69% in 2022.”
That’s a fairly massive jump in one year. The Google AI links also led me to this commercial marketing report which includes consideration of AIDS:
Somehow the Google AI comes up with a number of 80% of UK T1s “now using” a CGM. I couldn’t find that number but it’s clear from the commercial report (which is not scientific and has no references) that AIDSes are next on the horizon for the tech bros.
I found this US figure:
- “In a follow-up survey of > 1000 adults with T1D from the T1D Exchange, about 90% were using CGMs and two thirds were using AIDs.”
I regard that as hokey; I would expect a far higher proportion of use amongst T1s subscribed to t1dexchange.org, or TuD or FUD for that matter. It might be interesting to do a poll on BeyondType1 and then compare it with polls on TuD and FUD. Something like:
- Are you (or for parents your child) a T1 or T2?
- Do you treat diabetes using insulin?
- Do you use a CGM?
- Do you use an insulin pump?
- If yes to 2-4, do you use an automated system which delivers boluses (meal or correction) on the basis of the CGM readings.
Note that I’m trying to exclude low-glucose-suspend automated systems without using any technical terms (other than “CGM” and “pump”) because LGS systems aren’t AIDSes.
3 Likes
“Hybrid Closed Loop” systems use the CGM data along with carb estimates to handle both correction and prandial boluses.
“Full Closed Loop” systems do not use carb estimates; carb intake and prandial boluses are derived from “unexpected” BG rises.
“Leaning” systems learn basal and/or bolus amounts by studying trends over some time period. The bolus learning adjusts the “IC” ratio, insulin sensitivity, using a 24-48 hour period. This is an integral part of Loop. Basal was always available manually in loop by downloading the data into an offline program however my results with that sucked.
The terminology is imprecise. “Hybrid” and “Full” closed loop systems aren’t really different when the system adjusts insulin sensitivity and responds to elevated BG; the only difference between a meal bolus and a correction bolus is that the second happens later. A T1 on a keto but non-OMAD diet is unlikely to notice any difference in TIR and probably not in HbA1c as a result of not entering carbs.
3 Likes
I was not aware that DIY Loop automatically learns/adjusts IC or sensitivity. I’m using Loop, and I thought it only used the exact static numbers that I set for carb ratio and insulin sensitivity.
3 Likes
Our DIY loop doesn’t do this. We should be specific into which have this capability. With Omniloop, you have to manually adjust all the settings. Loop doesn’t “learn and adjust” on its own. I watch for patterns and tweak ISF, Basal, I:C, etc, by myself. I kind of don’t like the idea anyway of changes occurring without me making them. ![]() I’d never be able to keep track of what tweak is working and which wasn’t. When I tweak, I change one thing at a time and watch outcome.
I’d never be able to keep track of what tweak is working and which wasn’t. When I tweak, I change one thing at a time and watch outcome.
6 Likes
Hi allison. I also have the Tandem pump. I do go on extended pump breaks then go back on the pump until I get tired of it. I do like MDI more than the pump, but sometimes the pump makes sense. Like going on vacation.
4 Likes
I Use a Medtronic 770g pump and do finger stick 6-8 times a day. Yes, I am a dinosaur, but I’ve been Type 1since 1958. Unless I lose my eyesight I plan on staying with what I have.
7 Likes
I would be interested to 1) participate, and 2) see the results. This is a special group of people and not a random poll. I would be interested to know what people here are doing.
Possible questions:
- do you use a pump & CGM in an AID system (Automated Insulin Delivery) for basal & correction dosing? (yes/no)
If yes, go to question 2a, if no go to question 2b
2a) do you also bolus for meals, or is your system fully automated? (radio buttons)
- Bolus for meals
- Do not bolus for meals
Go to 3a.
2b) how do you manage your diabetes? (short answer)
Go to 3b.
3a) what pump and CGM do you use? (short answer)
Go to 4a.
3b) why do you like this system? (short answer)
4a) why do you like this system? (short answer)
3 Likes
I did a very simple poll ‘cos I did not see options for multi-question polls. Gotta look into that more.
6 Likes
Yes; I think I was mistaken and that it is a part of OpenAPS I had thought OpenAPS derived from Loop; so substitute “OpenAPS” for “Loop” in my previous comment. In fact it is the other way round; Loop was derived from OpenAPS, possibly losing insulin sensitivity calculations as a result. Here’s some history:
https://medium.com/@loudnate/the-history-of-loop-and-loopkit-59b3caf13805
And here’s an OpenAPS/Loop comparison:
Here’s a screenshot (from AndroidAPS, now called AAPS) which shows the sensitivity options:
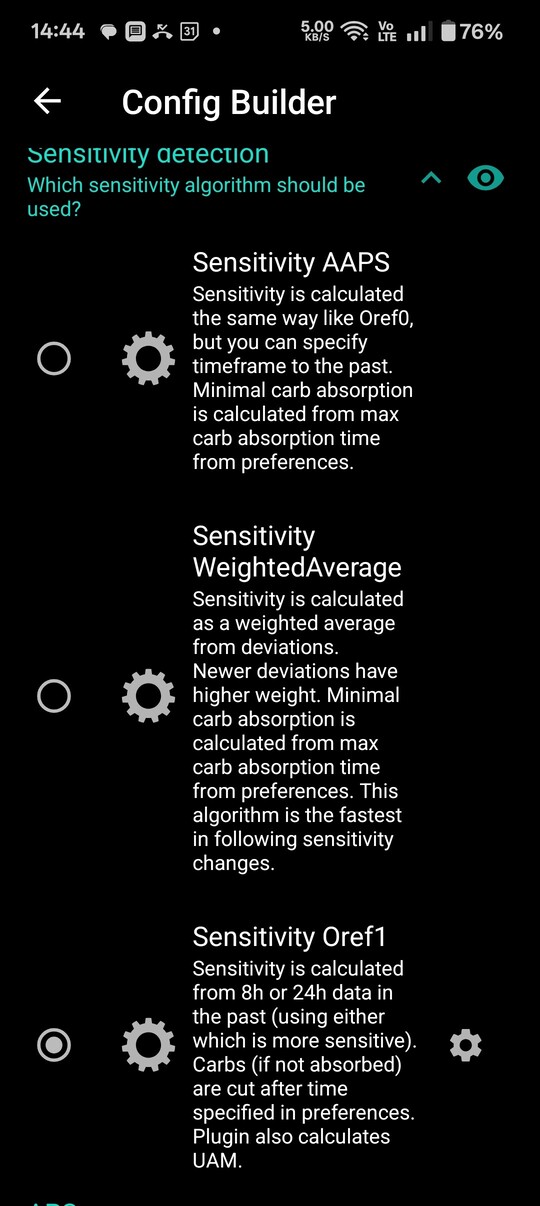
“UAM” is “Un Anticipated Meal” (yeah, not a good TLA). I believe the sensitivity affects the correction factor and basal but doesn’t override the manually entered values from the “meal calculator”. The precise details are in the documentation, somewhere ![]()
So stuff done via the UI, prandial and correction boluses entered via the “calculator” is, by default based on the numbers programmed in. However the default can be changed ![]() I’m using oref1 and the default. Here’s the screenshot for the “Dynamic ISF” option which is, basically, the “Full Closed Loop” option:
I’m using oref1 and the default. Here’s the screenshot for the “Dynamic ISF” option which is, basically, the “Full Closed Loop” option:

There are lots more options visible when it is turned on.
The OpenAPS reference design does do some sensitivity adjustment automatically, see “Adjusting for unexpected BG deviation” in the link to openaps.org above. It’s pretty basic but it does adjust sensitivity.
The AAPS oref1 implementation when “Dynamic ISF” is switched on uses the base calculation to affect everything. Here’s what happens on the AAPS home screen after I turn it on:
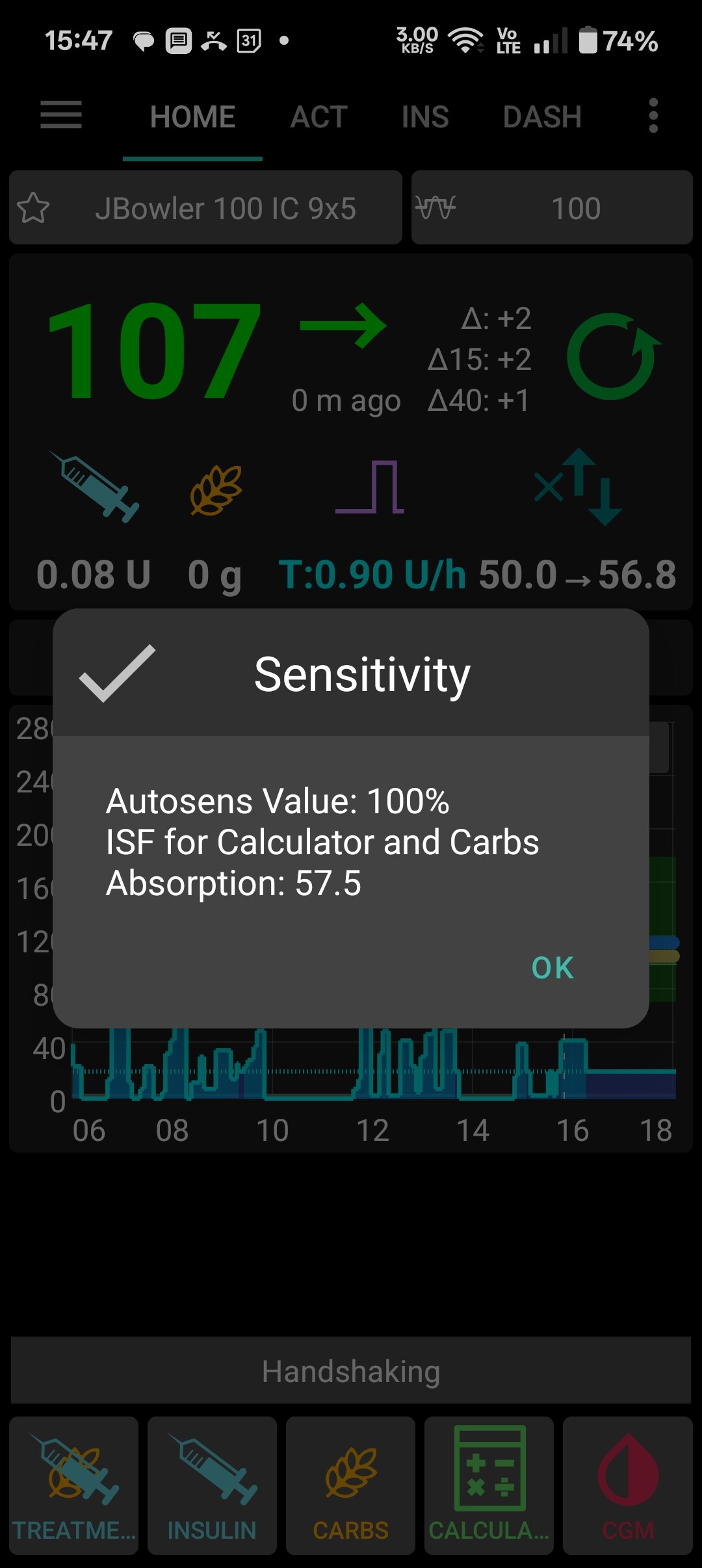
Look at the iconography immediately above-right of the pop-up. Dynamic ISF has adjusted my insulin sensitivity from 50mg/IU (the programmed value) to 57.5mg/IU. This is not unreasonable since I just spent several hours chainsawing and moving firewood.
3 Likes
For those that missed the poll, here it is:
1 Like
I went with Twiist because it is built upon an old version of Loop and is FDA approved.is it perfect? No. But it works well enough.
4 Likes
@bpollina - I’d love to hear more of your Twiist experience. I’ve used DIY Loop for nine years now and I’m happy with it but as I age I’d love to find an FDA approved commercial system that can work for me.
3 Likes
This is correct.
Omnipod 5 uses machine learning (if you are not running in manual).
Loop has no machine learning.
1 Like
Absolutely. Hang on. This could get quite long. Hope it helps someone.
Formally I’m an insulin dependent Type 2 diabetic because while my pancreas is all but dead, it still produces SOME insulin, and there are NO antibodies, so I have nothing auto immune going on. But I’m definitely insulin dependent, so treatment wise, I’m more of a Type 1 than 2.
Latest Labs:
A1C 6.0 on 11/19/2025
4/7/25
GAD65 <5.0
IA2 Antibodies < 75.
Anti GAD 65 < 5
2/6/25
Insulin Autoantibody < 0.4
ISLET CELL AB SCREEN NEGATIVE
I’ve been doing either LOOP or Trio for quite some time using Dexcom G7 and the Omnipod DASH and have loved it. I have it going to nightscout so I can have a tab open on my work laptop. I’ve used Sugarmate in the past as well. I’m a technology junkie.
So when I heard that Twiist was coming out, my endo didn’t originally want to write the script because it hadn’t been approved for Type 2’s and unsure if it ever was. I talked to the rep, and she said that it was through the prescription side so no proof of 1 vs 2 needed and no documentation needed. It went right through 100% no copays just like the G7 and Dash did. The only problem we had was the Libre 3+ wasn’t on formulary, so we had to try twice for a prior authorization. All it took the second time was them saying that the pump only works with this CGM and no others. I hear they are eventually working on getting the G7 onboard, but right now they are working on the Eversense 365 by Q1 2026, and I”m seriously thinking of going that, but would need another prior authorization.
The Libre 3+ is great when it works but horrible when it is not. The 2 things I don’t like is that its only 1 channel, so can’t do things like nightscout or any other API stuff, and second it cannot be calibrated, so if you get it on a bad spot on your arm and have false lows, you basically have to ride it out and hope it starts to correct itself or pull it. But once it gets going, it does last the entire 15 days, so that’s good. I’ve never had much luck getting the G7s to last the entire 10 days. Usually it would go wonky around day 6 or 7.
The twiist is super easy to use. The pump itself is about the size of a small yoyo that can fit in your pocket, in a belt clip they give you or jury rigged to fit on your body. Unfortunately it is NOT water proof, so you can’t shower or swim with it. And I’m not sure I like going backwards with tubing, but I’m getting more and more used to it.
Inserter wise it uses the Cleo which is absolutely a NIGHTMARE! It’s a manual inserter that always seems to pull off when you pull the inserter away from the body about 1/2 the time, so you waste a lot of them. Fortunately if you call their support line they replace every one of them. often times they will just ship you a complete replacement KIT with everything. Their support line is excellent btw. All US based and they don’t read off a script. They actually listen!
They are supposed to be developing their own equivalent to the Cleo but that’s down the road. It uses a proprietary version of Lure Lock, so not many will work, and those that do people are having problems getting sourced from DME places.
Software wise, it looks nearly identical to LOOP. It is actually an older version of LOOP with certain things missing like overrides which I didn’t use and remote bolusing which I didn’t use either. It does have an exercise mode though.
It also seems very aggressive and keeps my numbers in check very well without too much deviation.
But the best part that made me pull the trigger and I think will for QUITE A LOT OF PEOPLE is that since it is prescription side, there is absolutely NO COMMITMENT! Try it, and if you don’t like it, just don’t fill the refill kits! No other AID system that I’m aware of that’s FDA approved does this!
Hope this helped someone! If you have any questions please ask away!
5 Likes
This is a great way to ask the questions, but I have never seen anyone run multistep (conditional) polls before. I don’t think you can do it. It would be cool if you could.
2 Likes
Thanks for the review, @bpollina. I like reading the experiences of actual users.
There’s a flip side to the Rx only side of insurance coverage. Sequel’s decision for Rx only works for people like yourself who wish to trial the system, but people on Medicare can’t use the DME benefit to pay for the Twiist. And the Medicare Part D Rx I can buy has no coverage for Twiist. That keeps me on the sidelines for this product unless I want to pay 100% out of pocket.
In the meantime I’ll continue to pay attention to users like yourself. Even if Sequel began to accept Medicare DME, I would wait until Dexcom or Eversense CGM became approved since I think the Libre 3+ would not work for me. An Eversense CGM that lasts for one year looks like an attractive solution.
Good luck with the Twiist! Report back when you can.
4 Likes