Yes I have thyroid disease. I have had that disorder for 20 years now. T1D. Whenever I have had to go up in dosage on that it had never effected my basals before. I am not going to rule that out though since our bodies seem to change all the time.
Could be a mechanical problem with the pump. I usually need a new pump every 4 years. The last time I just had to switch back to vial syringe when the pump was not functioning properly, until the insurance would cover a new one. I called the company to trouble shoot it, but they said it was fine.
You could try vial syringe/ insulin pen to rule out a mechanical problem.
Make sure you have some long acting on hold at the pharmacy.
Do you need a change to you carb ratio? Auto mode has limitations to how much it can help. If you are seeing post prandial spikes, this would be a sign of needing a change in the carb ratio.
I am in manual mode and my radio is 1:7 and active insulin is 2 hours the lowest it will go. So ratio seems to be working great. It’s when I haven’t ate anything and still stay higher. If I use AM I am always in the high 200 low 300’s so I stay away from AM.
Hi Ashly. No question your thyriod and use of Synthroid to help cover the shortage of thyriod is playing a role here. One thing i noticed that you mentioned was that in the past when you increased you synthroid dose it never effected your basals. In general for most people your Total Daily Dose of Bolus and Basal will be about the same, so if your increasing your bolus amount your basel will need to also increase. When i was using a pump i used to take a 3 day avg of my TDD and divide it by 2 to calculate my ideal daily basel amount, then multiply all my current rates by a factor to bring my total daily basel dose up or down to this new ideal basel amount. If a lot of pump users did something like this in excel weekly they would have vastly better blood sugars. Instead what happens is people don’t do this for various reasons and say they’re taking 30% Basel and 70% Bolus and they wonder why the universe has it out for them.
Good point! I have never done the excell math thing to figure out basal so I’ll have to try that. My A1C is still super good. 5.2 2 months ago and I’ll find out in a couple of weeks again what it is. Looking at my summary my basal Friday was 52% and my bolus was 48%. Thurs was 55% and 45% Wed was 39% and 61%. Most of the blouses on Wed were corrections. That’s when I upped my basal again. Which made it back to pretty close to 50/50. I am now intrigued to see if I can figure it out. I am bad at math but want to see if I can do this…
So I get the 3 day avg of my TDD and divide it by 2 to calculate my ideal daily basel amount, the part I am confused about is this… then multiply all my current rates by a factor to bring my total daily basel dose up or down to this new ideal basel amount. Can you give me better detail how to do that? I appreciate the help!
My experience with thyroid disease (Graves’ in my case) is that low thyroid had no real effect on my insulin needs that I could find beyond the normal variations. But high thyroid made my needs increase dramatically and that, as well as the process of my thyroid coming down from high to normal, was utter blood sugar chaos. Truly uncontrollable.
My blood sugar overall was more volatile and difficult to control while my Graves’ was active (compared to now in remission). But it was only crazy high while my thyroid was high.
I would like to dispute this line of reasoning. Can you cite any proper scientific results that show “most people” have approximately equal requirements of basal and bolus insulin, or that there is any benefit to adjusting basal and bolus so that the amounts are about equal to each other?
For each person, the basal requirement is whatever amount is required to keep the BG roughly stable in the absence of other factors (such as food, exercise, illness, hormones). The reason to change your basal is if your BG has a tendency to rise all by itself then you need more basal, and if your BG has a tendency to fall all by itself then you need less basal. It’s as simple as that. Nobody else’s basal information has any bearing on the amount of basal your own body needs.
For each person, the insulin:carb ratio is the number of grams of carb that are correctly treated by 1 unit of insulin. So, for instance, 1:7 means if you eat 7 grams of carb and take 1 unit of insulin, then (given a correct basal and no other factors like stress, illness, exercise, and so on) your BG after around 5 hours will return to the level it was before you ate. This also is simply a property of the body, and we need to take whatever amount our individual body needs to cover the carbs we eat, and the insulin:carb ratio of any other person’s body is totally irrelevant.
So our daily total bolus insulin is pretty directly determined by our insulin:carb ratio and the number of grams we eat on any given day.
The ratio of basal to bolus insulin is determined by your body’s basal requirement, your body’s insulin:carb ratio, and the amount of carbs that you eat. I’ve never seen any study that even hints at any benefit to changing the amount of carbs you eat in order to reach a 50:50 ratio of insulin to carb. There is no “better” ratio of insulin to carb, it just is whatever your body needs for what you eat.
@bkh I completely completely agree with all of this. Everyone’s needs are different, insulin intake is going to depend on one’s own body and needs. I’ve seen this 50/50 statistic floating around the last couple of months on other forums, I believe it’s BS. I just checked my 7 day average on my X2 and my basal to bolus ratio split is 38/62. My avg BG is 121 which is exactly where I want it. Am I a fool or don’t know what I’m doing because I don’t have a 50/50 basal to bolus intake?
Hi bkr. I wasn’t talking about bolus to carb ratios. I was talking about the basal to TDD ratio. I think the easiest way to understand this is having a look at the Tidepool graphs i included, you can the median basal ratio’s for adults are somewhere around 48-52% of the TDD. If you consider that in general the people who are nice enough to donate their pump information to tidepool are in better control than the average diabetic out there its useful information.
There are papers as well, sometimes its 48%, 49.5% etc. I just found these, kind of limited reading though. I found very detailed papers in the past where they’ve said something like 48.5% had the best results. https://www.ncbi.nlm.nih.gov/pubmed/20920437, https://www.ncbi.nlm.nih.gov/pubmed/19158048
This isn’t some hard rule though. However if she is running high i would say this is an obvious thing to look into and possibly adjust if her blood sugars are running high. I’ve been a type 1 for over 30 years and was on a pump for over 20, i found i was in the “zone” being around that ratio.
It sounds like you are managing your changing landscape just fine, IMO. I would caution to be careful about applying statistical rules of thumb when what you’re doing doesn’t seem far off the mark. Since you’ve got some specific health concerns to investigate, I would personally look there first before adopting a new method of deciding on dosing. Just my opinion with an interest in safety and prudence. YDMV. (My basal bolus split is 30/70 which is close to what one might expect for my body type per “Think Like a Pancreas”.)
The second paper is behind a paywall, so I can’t evaluate it. But let me summarize the first paper, which I find remarkably naive. Their data set was the anonymous pump settings from 2007 for about 1000 Deltec Cosmo pumpers. Looking at the data from the 1/3 who had the lowest BG (average 144 mg/dL) they observed that the average basal setting was 48% of the total daily dose of insulin. Based on this, they proposed that it would be best for everyone to set their basal insulin to 48% of their total. Similarly, they proposed that for best results, everyone should set their carb ratio to 2.6 times their body weight in pounds, divided by their total daily insulin dose. They had another qualitatively simple formula for setting the insulin sensitivity.
Their conclusion about these proposed formulas is “We have developed a model with the hypothesis that improved glucose outcomes will result from the use of formulas to derive appropriate pump settings. Prospective validation of these concepts is needed.”
In other words, they made up some exquisitely simple formulas for setting basal and carb ratios and insulin sensitivity factors, based on the average values that some pump users were using in 2007. They hope that these formulas would give the best pump settings for everyone, and they suggest that an experiment should be run to see if they do. They show no evidence at all that setting your basal to 48% of your total daily dose is a good thing to do.
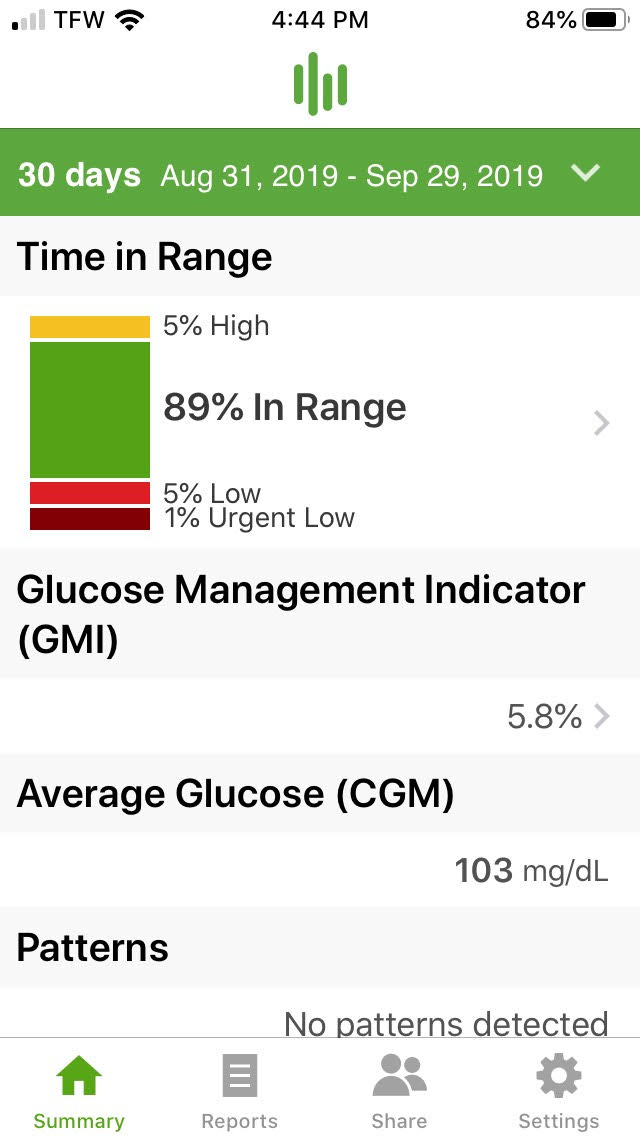
Hi bkr. I misread one of her replies, i thought she was saying she never raised her basals rates in the past due to the thyroid medication, I interpreted as she wasn’t increasing her rate, and hey if your running high all day its kind of obvious your basal rates are likely not correct. The Basal/TDD Ratio is very important, that’s why I brought up that as a suggestion. I don’t know all the details of her background, how long she’s had diabetes, weight, etc. Typically an endo will use the 50/50 split as the suggested starting point. I hope I didn’t come off as saying that’s some sort of universal law, people should do whatever works best for their situation. I was on a pump for 20 years and never had a sub 6 a1c. If Ashly has a A1C of 5.2 that’s fantastic, what could a clown like me offer in way of advice. I personally dumped the pump because of absorption issues and it was about $3-$4k cheaper for the insurance. Sam on this board was one of the people who changed my mind to try something different. Switched to Tresiba/Afrezza/G6. I spend a fraction of the time i did before and its just way easier. Here’s my last 30, i was getting even better results at the start when i more effort into it.
For the TDD average add all days and divide by the number of days then take the total and divide by 2. The 1st half is the basal and the second half will be the boluses divided among 3 meals.
To see if the basal is working you can skip a meal and see if the glucose remains the same or goes up or down. This helps determine if it the basal or bolus that needs to be changed. Active insulin time is 2 hrs? Are you requiring a lot of post meal correction? The usual active time is 3 hrs or 4 hrs.