So, I went back to see the diabetes educator after having the g5 for the first 2 weeks, and I got really frustrated with being told that on 2 weeks of data, I should be increasing my night time Levemir when it generally drops me around 10mmol/L overnight.
I have had many issues with my HCP’s basically calling me paranoid about hypos (why wouldn’t I be when I’m hypo unaware and I live alone) and that it’s the reason for my many DKA’s (FYI none for 8 years and that’s because I realised that stress was my nemesis and no longer work).
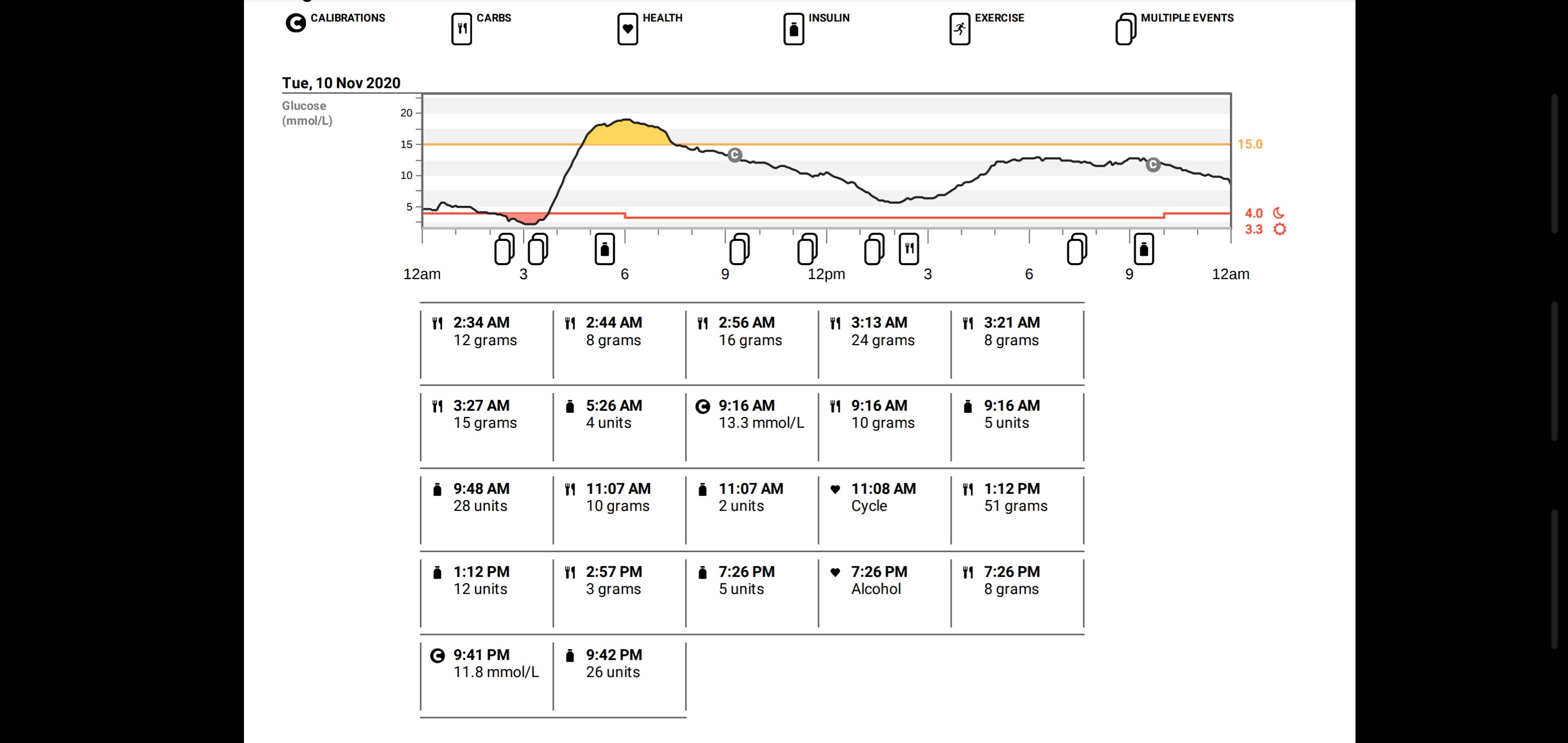
So, I increased my night time Levemir by 2 units. I had a small snack to bump me up as I was 7.2mmol/L before bed.
At 2:30am the urgent low alarm woke me. I usually don’t need many to bring me up, but it took an hour of constant alarms and subsequent jelly babies to start to make a difference! Of course, then they all kicked in at once and at 5:30am I needed to correct after topping at 18.3mmol/L. It even got so low that the g5 would only say low! Screenshot_20201113-174744_Drive|690x326
Needless to say, I’ve readjusted my dose, and I will just smile and nod at future DE’s that think they know what my body is going to do. It just really frustrates me that you go to these people for help and insight, and they don’t take into consideration, our individuality.
My impression is that diabetes educators like to look at no more than the last two or three weeks of data, spot trends that in fact aren’t there and then recommend unnecessary dosage adjustments. Dropping 10 mmol/L (or 180 mg/dL for some of us) overnight really is a lot. You’re right to readjust your dose.
My endo does the same thing - just reviews a couple weeks’ worth of data and suggests tweaks to my settings. She was bothered that I made changes to my pump between visits (which are, admittedly, farther apart than they’d like them to be) - I understand a bit, because as she said, she is responsible if something happens to me. But really, it’s frustrating because I deal with this every day and I know what is happening every day between those visits to their office. I feel ya.
Time for a new endo in my book, at at least a conversation at your next visit. You are the best captain for the ship, not the person that steers the ship once every few months.
Unless you have a habit of making things a lot worse, I don’t understand why an endo would object to patients making changes. The responsibility thing I don’t understand either, what if something happens when you don’t make changes? What if a change could have prevented that?
Do they have a good reason why they would like you to visit more often? Unless there are certain issues that require their attention, there’s no need to visit them frequently. I don’t see my endo more than once a year. He only asks patients who need more help to visit more often.
Thanks for that link @CatLady ! I was surprised to read this sentence ; “In most cases, the daily (24-hour) dose of basal insulin is slightly less than the daily mealtime insulin.”
Here in Australia, we are told that our basal should be around 70-75% of our daily insulin. I’ll be giving that test a go.
I am all for taking control of my treatments, but it will always be frustrating that I end up doing it all myself anyway. I often wonder what the point of these appointments is.
I’m with the other commenters here @allison . I don’t see my endo any more than once a year now I’m ‘stable’ (I also have thyroid issues that went from Hashimotos to Graves disease and then back again).
I hadn’t seen an educator for years, until I was put onto a cgm. I see an endo again in March, but that’s because he wants to see what difference there will be with the cgm, plus he probably wants to check out my overnight drops.
I find it interesting that your endo says it’s her responsibility if something happens to you. That must be so stressful feeling so responsible for all of your patients like that.
Thanks @Boerenkool. Yes, the major drop overnight has been a big concern for me. It’s also the reason I was convinced to give the cgm a go. I am really affected by temperature changes and of course so is insulin so I have always had to do seasonal changes, but, this year my normal changes haven’t worked so well. Even with the smaller night dose of Levemir, I am still getting the major drops. I’m going to do the basal test that CatLady posted in the thread, and see what that tells me.
Good question. Their standard of care is every 3 months. That’s how it has been my whole 25 years of having diabetes! I definitely don’t need to go that often so I stretch it to 4-6 months if possible. Otherwise it’s truly a waste of money. (This is at what rhymes with “Believeland Clinic.”)
Yes, I can’t imagine! I wonder if it’s concern that she will get sued or something? I’ve only seen her a handful of times as I have had to switch when I’ve aged out of pediatric care, moved, etc. She’s nice enough though. I think she’s a young doc so maybe still following the books closely? Idk.
Oh I know! I have made tons of adjustments over the years on my own. It’s been 25 years and I have no complications. I think it was an off-handed kind of comment; maybe she doesn’t want to get sued. But ultimately I am making the decision for myself - I have made plenty of changes to my settings since I saw her last
That’s the standard of care in many places and I was so used to it, but my current hospital has encouraged me to come less often, because there isn’t much they can do for well-controlled patients who are capable of managing their disease on their own. If a problem should arise, I can still call them or make an appointment.
Similar for me, I have been going 2x per year. Will be 3 times this year due to new endo and switching to tandem pump, and switched due to her experience with tandem users. Prior endo was a medtronic only club, and treated more T2s.
Why does an endo have an aversion to cgm data? That seems really odd!
I have only been seeing my endo annually as well, for the past couple of years. If I’m having issues it’s more often, but I’m aware that seeing one via the public health system (Australia), means that they will have a large number of patients on their books and so if you aren’t having problems with things, then they are fine with only seeing me once a year. My GP sends them copies of all my tests anyway, so if they need to see me, they’ll let me know. Besides, my GP is fantastic.
@SBee, I feel for you too:( Weirdly, we have had better relations in the past with educators than with endos. Our endo relationships have sometimes been fraught with conflict, as, at times, the endo feels that she/he knows more about our diabetes than we do (and, of course, it is sometimes true!). We have found diabetes educators to be T1s much more often than endos, and much better at understanding daily realities… Possibly look at another educator in the practice?
Btw, have you considered closed loop options? If the tandem pump is not available where you are, possibly OpenAPS or Loop? I understand that you are on MDI right now. For us, switching to Loop (however imperfect) for my son has made a world of difference to nights.
@Michel , it used to be the same for me too. My endo and I tolerate each other, but I will always think he’s an arrogant ass, and he probably considers me insolent. I also have thyroid issues that he sees me for, and a number of years back I knew something wasn’t right and when I asked him about it, he told me that I was looking for problems, so I went off my thyroid meds and turns out I was right! My body had gone from being underactive (Hashimotos) to being overactive (Graves disease), and then I spent the next 3 years on anti thyroid meds. But he’s never admitted that I was right and he wasn’t.
Because I am in the public health system, I don’t have a choice in who I get to see, whether it be an endo or educator. I am thankful for universal healthcare however, so I deal with whomever comes my way. Besides, my endo is too far up the chain of command to see me now I’m stable in both my diabetes and thyroid. He leaves that to either the registrars or some of the newer endos on the team.
I am on a disability pension, so a pump and the consumables are something that I just can’t afford. While the CGM has been fully subsidised for me since March, pumps are not yet. Besides which, I am not comfortable with being attached 24/7 . I am starting to struggle with the CGM to be honest, but I will persist with it purely because of the valuable data.
I have changed up a bunch of things in relation to my insulin. I’ve changed my i:c ratio for lunch and afterwards, and I have also increased my morning Levemir and reduced my nighttime. I am on a split dose because it ran out on me always, so I wondered if my morning dose was doing similar. So far, the changes have been promising. I won’t see the endo until March, so it will give me plenty of time to play with things and get it all working for me better.
@SBee My endo is old school, and believes the only way a type 1 can achieve non-diabetic (normal) BG and A1C’s is by constantly having lows to offset the highs.
Given that Canada also has a public health care system, there aren’t a lot of options for endo shopping
My first endo was a jerk and after a few visits I refused to go back to him.
Did she want you to up your dose at night because you are waking too high or???
I used to drop a pretty good amount when I first went to sleep, so I would start higher to make up for it and then I would be high when I woke up. But it turns out I had DP and my basal was actually too high. A CGM and a pump solved most of my issues. But I know people on MDI that just automatically take some insulin when they first wake up or they actually set an alarm to take some in the early morning hours and go back to bed.
I find I can go into a new trend very easily. Over the years, I have had drops at night around 1 am, to going high at 1 am. DP and then no DP, FOTF and DP to then nice smooth sailing. Who knows why things change but they seem to periodically.

{kind=link}